
Dr. K Sharada Reddy, Author
Senior Dentist & Full Mouth Rehabilitation Expert
Teeth loss is a very serious problem that impacts overall health. There was a time when traditional removable dentures were the only treatment option to rehabilitate a complete set of teeth.
Dental implants were introduced in the early 80s to replace missing teeth, hold prostheses securely in place, and provide a stable solution for teeth replacement. With the introduction of dental implants, embarrassing moments with wobbling dentures were effectively managed. A dental implant is a post made of surgical-grade titanium, designed to replace a tooth along with its root, thereby preventing bone loss, which typically follows tooth removal.
Replacement of teeth using conventional two-piece implant systems in the early days often required additional surgical procedures like sinus lifts. These procedures were necessary to elevate the pneumatized sinus floor, which often occurs due to long-standing infection or when teeth are missing for an extended period and not replaced, particularly in the upper premolar and molar areas.
In such instances, the bone present below the drooped sinus may not be sufficient to support even a minimum-sized 6 mm implant. That is when invasive surgical procedures like sinus lifts are performed to elevate the sinus to its original position. Bone graft material is then added under the sinus and left for a few months until the grafted bone integrates and hardens enough to support an implant.
Thus, the conventional method of implant placement involved multiple sittings and was quite invasive, with long waiting periods before permanent teeth could be fixed on implants. Furthermore, these implants were not recommended for diabetic patients and smokers.
Basal implants, also known as single-piece implants, were initially introduced to provide immediate teeth-loading solutions for patients with atrophic jaws. As the name suggests, basal implants are placed in the cortical or basal bone, which is located adjacent to the alveolar bone that holds the tooth roots. The basal bone is highly mineralized compared to the alveolar bone. When basal implants are placed in this highly mineralized bone, they allow for immediate loading of teeth, though the implants only achieve osseofixation (a mechanical bond) rather than true osseointegration with the bone.

On the other hand, conventional implants were placed in the spongy alveolar bone rather than the basal bone. This placement caused a delay in osseointegration with the bone, thereby extending the process of teeth fixation by several months.
An advantage of basal implants over conventional implants is their ability to support immediate loading of teeth, even in cases with minimal bone, without requiring additional surgical procedures. However, there are some downsides to consider:
DISADVANTAGES OF BASAL IMPLANTS:
- Basal implants are designed as a single unit, where the implant body and the abutment that supports the crown are fused together. This design makes it difficult to adjust the inclination or angulation of the implant at the gum or gingival level for a favorable prosthesis. The only possible approach is to bend the implants at the gum level, which is feasible only if the torque (tightness) of the placed implant is above 60-70 Ncm. Otherwise, the entire implant may displace from the bone, and in some instances, the bone may crack due to the pressure exerted while bending.

CONVENTIONAL IMPLANTS
Conventional implants, being a two-piece system, consist of two individual units: the implant body, which is embedded in the bone, and the abutment, which supports the prosthesis and forms a connecting link between the implant body and the crown or bridge. The main benefit of this system is that, regardless of the angulation of the implant in the bone, it can be comfortably corrected at the gum level using a multi-unit abutment, which is available in various heights and angulations.

- The non-availability of larger diameter implants, the compromised strength of basal implants, and the mode of implant integration with the bone (osseofixation) necessitate increasing the number of implants per jaw for a full-mouth reconstruction using basal implants. The minimum number of implants required to replace an upper and lower arch with basal implants is around 10 implants per jaw.
Full-mouth rehabilitation using conventional implants can be achieved with the “All-on-4” or “All-on-6” concept. In the “All-on-4” approach, four implants are placed in each jaw to secure a hybrid denture. The “All-on-6” concept requires six implants in each jaw to support a full set of DMLS or zirconia on a titanium frame fixed to the implants. The “All-on-6” concept is preferred over “All-on-4” as it avoids cantilevers in the prosthesis and provides a more stable, long-lasting solution.
- Another major disadvantage of basal implants is that the prosthesis must be cemented onto the implants. In other words, the bridge is glued to the implants, which complicates retrieval if needed. The prosthesis, whether an overdenture or a bridge made of PFM or zirconia, is prone to wear and tear and might require replacement. The lifespan of an overdenture is around 4 to 5 years, while a zirconia bridge, though strong and durable, can still experience accidental chips or cracks that require repair. Removing or separating a cemented bridge from the implants is difficult and hazardous, as the implants osseofix with the bone. Thus, the removed bridge will be damaged and cannot be reused; it must be replaced with a new one, which can be costly. Additionally, if any cement escapes into the gum tissue during fixing, it can lead to gum inflammation and bone loss.
On the other hand, conventional implants are screw-retained, meaning the bridges are fastened onto the implants with screws. If any issues arise with the prosthesis, the screws can be easily removed, repaired, and the same prosthesis refixed within a day or two.
- Basal implants osseofix with the bone, whereas conventional implants osseointegrate with the bone. Osseofixation involves a mechanical interlocking between the bone and the implant threads, while osseointegration involves bone cells multiplying and growing around the implants to fuse with them, providing a stable connection. Osseointegration is critical for the success of an implant.
Due to these disadvantages, basal implants are not approved by the US FDA and are not recommended in countries like Australia, the United Kingdom, Canada, and many European countries. Therefore, basal implants are not suitable for international patients traveling to other countries for fixed teeth on implants.
What should be the treatment of choice for international patients who want to avoid additional surgical procedures, lengthy waiting periods, or the complications associated with basal implants but still achieve fixed, permanent teeth immediately in a single visit and, above all, have a universally accepted screw-retained prosthesis?
It is well known that conventional implants have several advantages over basal implants, with some exceptions such as:
- Delayed loading (waiting 3 to 6 months before teeth can be fixed on the implants).
- Requires additional surgical procedures like sinus lifts and bone grafts.
- Risk of peri-implantitis.
- Not suitable for diabetic patients and smokers.
To address these issues, the CPBCCI Protocol™ has been introduced by Dr. K.A. Reddy, a certified implantologist at LBR Dental and Implant Center in Hyderabad, India.
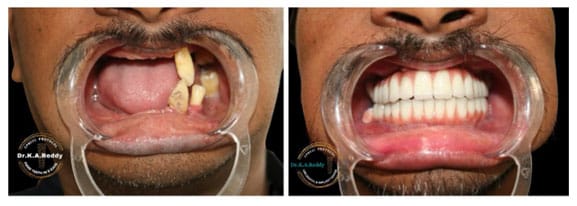
Dr. K.A. Reddy, a leading implantologist in India, is known for his expertise in both basal and conventional implants and conducts advanced implant courses for upcoming implantologists. He has successfully treated cases that other doctors failed to rehabilitate, including patients affected by mucormycosis (black fungus), a complication of COVID-19, where he placed implants and rehabilitated patients in less than a week.
He is chief mentor of Noris Implant systems, Israel. Though Dr. K. A. Reddy is well versed with the both Basal and Conventional Implant Surgery Systems, he prefers to use Conventional implants with CPBCCI PROTOCOL ™ as it has benefits of both Basal and Conventional Implant Systems combined together.
- The main issue with conventional implants is delayed loading due to their placement in spongy bone, which is less mineralized and requires time to osseointegrate. With the CPBCCI Protocol™, conventional implants are placed in the highly mineralized basal bone, allowing for immediate loading of the teeth.
- Another problem with conventional implants is the need for additional surgical procedures like sinus lifts and bone grafts. The CPBCCI Protocol™ eliminates the need for these procedures. In cases of severe bone loss with sinus pneumatization, implants are tilted at an angle of 30 degrees or more to avoid anatomical structures like the sinus and important nerves.
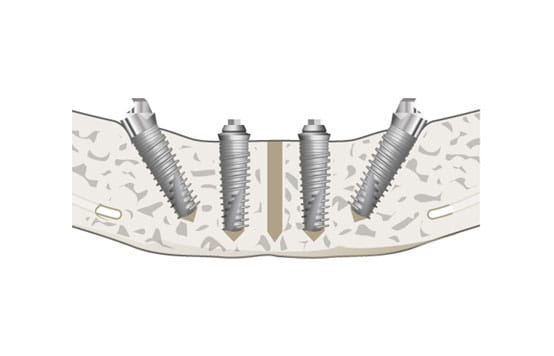
- If the height of the jaw bone is not proper, longer implants can be placed by tilting them at an angle there by increasing the Bone: Implants contact ratio which helps in increasing stability and provides additional anchorage to the Implants.
- Can engage the bone with good density.
- Can avoid long span of cantilevers in the prosthesis due to distal inclination of the implants in “ALL ON 4” cases.
- Uniform load distribution
- Quick recovery (no additional surgery)

Therefore the implants we use in CPBCCI PROTOCOL™ will counter both the problems related to infection and Osseo Integration there by making it safe to use in Diabetic, hypertensive patients and also in people who have the habit of smoking.
4. Peri implantitis, an infection that develops around the gum surrounding the Implants is another problem associated with Conventional Implants.
In CPBCCI Protocol ™ since we are using the multi-unit abutments on the implants, which in addition to straightening the implants at the gum level also maintain 2 to 3 mm distance between the implant body embedded in the bone and the prosthesis present at the gum level, thereby arresting the infection at the multi-unit level and safe guarding the implant. This is an additional precautionary step as the smooth surface present in the Implant will avoid peri implantitis.


Screw Retained Prosthesis :
As mentioned earlier the prosthesis will be screw retained which is the biggest edge of the Conventional implants over Basal implants.
Few Implant centers to cut down the expenditure incurred with the Multi-unit abutments, they use regular abutments and cement or glue the prosthesis on the Conventional implants instead of using the screw system which is one of the chief benefits of Conventional Implants. People undergoing Implant treatment should be aware of this.
When Conventional Implants are available with all the added benefits of Basal Implants and are Immediate loading ,then there is no reason to opt for Basal Implants which are not approved in US and in fact prohibited in few countries.

QUICK ENQUIRY

Success Stories

International Patients
Our Clinic

Share this post
Author
Dr. K Sharada Reddy
Senior Dentist & Full Mouth Rehabilitation Expert